Updated information is highlighted below.
CASE STUDY:
23-Year-Old African American Female With Shortness of Breath and Cough for 3 to 4 Months
IMAGING
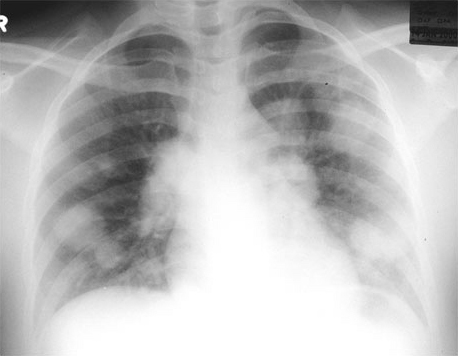
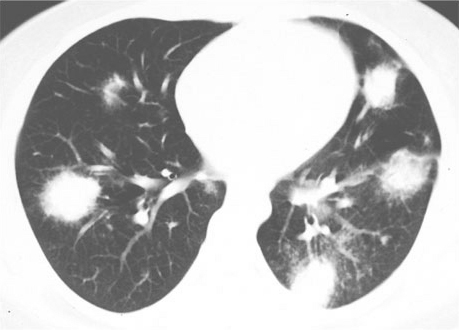
Radiology: Chest radiograph (Figure 1) shows multiple, large lung masses. CT (Figure 2) shows the masses to have poorly marginated edges. Small nodules, a few mm in diameter, are seen adjacent to several of the masses.
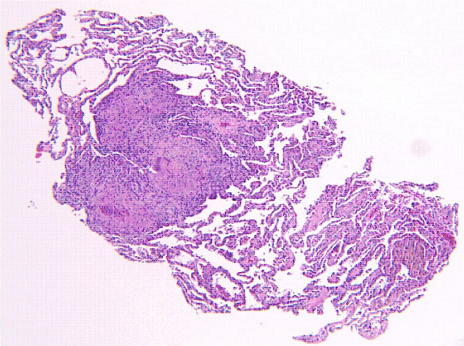
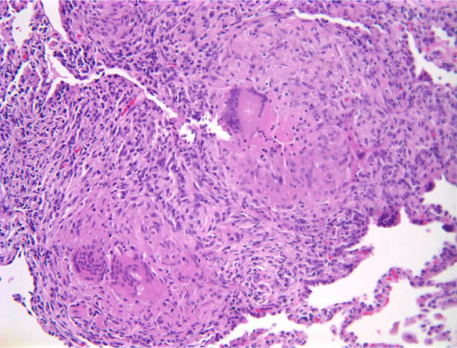
Pathology: The patient underwent flexible bronchoscopy and several transbronchial biopsies were taken. The biopsy sections showed alveolar parenchyma with small non-necrotizing granulomas (Figure 3). These granulomas tended to aggregate, as seen in Figure 3, with several nodules coalescing into a larger, rather discrete lesion. Also, there was minimal chronic inflammation around the granulomas and no inflammation extending out from the granulomas into surrounding lung parenchyma. These secondary features were useful in separating the granulomas of sarcoidosis from those associated with infections (where in addition, necrosis is commonly present). The granulomas of sarcoidosis typically have associated hyaline sclerosis (not evident here), but this finding was not a prerequisite for the diagnosis. At a higher magnification (Figure 4) several multinucleated giant cells were observed, another nonspecific feature. Sometimes distinctive inclusions can be seen in the granulomas of sarcoidosis (Schaumann bodies, asteroid bodies), but these are not specific for sarcoidosis. Whenever granulomas are present in a lung biopsy, the differential diagnosis is broad and includes infection, sarcoidosis, berylliosis, hypersensitivity reactions, pneumoconioses, certain lymphoproliferative diseases, aspiration, and even intravenous drug abuse. At a minimum, special stains for acid-fast organisms and fungi should always be performed.
|